Clinical Impact of the Tumor Therapy Manager
| Bernhard Preim | Otto-von-Guericke University Magdeburg |
| Jana Dornheim | Otto-von-Guericke University Magdeburg |
| Lars Dornheim | Dornheim Medical Images GmbH |
| Andreas Boehm | University of Leipzig |
Published: October, 2010
 |  | Full article |
Summary
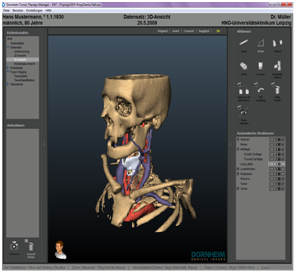
Visual exploration of CT and MRI datasets in clinical practice is still dominated by slice-based viewing. Volume rendering is now widely available but seen primarily as a tool for a fast overview, and only rarely as a visualization to directly support clinical decisions. Research projects aiming at advanced 3D visualizations, such as smart visibility techniques and illustrative renderings, usually fail to meet clinical demands, since the visualizations are not dedicated to specific diagnostic and treatment planning questions. Moreover, they are unfamiliar to users who need reliable and familiar visualizations as a basis for their crucial decisions. Discussions with clinical practicians reveal that the parameterization of such visualizations is too cumbersome and that resulting visualizations are often too complex. We describe and discuss long-term experiences on developing, testing, and refining image analysis and visualization techniques for ENT surgery planning based on CT data. While visual quality and a faithful rendition of spatial relations indeed are essential, it turned out to be superior to generate sequences of rather simple 3D visualizations directly supporting specific treatment questions instead of presenting many anatomic structures simultaneously. We report on the actual clinical use of the system and discuss how it changed the surgical planning workflow.
Impact on clinical practices
The TUMORTHERAPYMANAGER has been used for planning approximately 100 neck surgery interventions. In most cases, a selected set of functions was used to segment, quantify, and visualize the tumors in their spatial surrounding. In some 30 cases, the full set of functions – including the virtual endoscopy and the documentation functions were used. The computer-assisted planning process is performed in addition to the conventional planning process based on CT-slices. This is not necessary but serves to compare the different workflows. In approximately 10 cases, the 3D visualizations are employed in the tumor board for interdisciplinary discussions. In general, the surgeon feels safer with the computer-assisted planning and better prepared for surgery. Only, in rare cases however, he changes the surgical strategy with respect to radicality and access. The computer-assisted planning process is accomplished in difficult cases where the tumor disease is at a later stage and therefore treatment is particularly challenging (two out of three patients exhibit a tumor in the late stages III and IV, and ten percent exhibit metastasis). The system is used in one hospital although care was taken in the task analysis stage that it is not overly specialized for this specific setting. The TUMORTHERAPYMANAGER is considered particularly useful for planning treatment of surgical interventions at the larynx. This is because all relevant target structures (cricoid cartilage, thyroid cartilage) can be segmented and discriminated well. With respect to tumors in the oropharynx, not all relevant structures can be separated and thus the 3D visualization is less helpful. Primarily, one surgeon, a co-author of this paper, employs the system and describes that he appreciates particularly, the precise documentation function. This allows for the first time to communicate precisely the findings of the panendoscopy, in particular the estimated depth-infiltration of vascular structures and other tissue . He reports that with these functions he is more careful in the endoscopy since more findings can be reported.
Copyright of article and images belongs to the author or his employer unless otherwise mentioned